To be sold on retail on prescription of a Registered Medical Practitioner only.
Prescribing Information
1.0 Generic Name
Amoxycillin and Potassium Clavulanate Tablets
2.0 Qualitative and Quantitative Composition
Each film coated tablet contains: Amoxycillin Trihydrate IP eq. to Amoxycillin…………………………….500 mg/875 mg Potassium Clavulanate Diluted IP eq. to Clavulanic Acid…………………………………..125 mg Colour: Titanium Dioxide IP
3.0 Dosage Form and Strength
Film coated tablet Amoxycillin and Potassium Clavulanate (500 mg/875 mg and 125 mg)
4.0 Clinical Particulars
4.1 Therapeutic Indications
For the treatment of bacterial infections such as sinusitis otitis media, tonsillitis, acute and chronic bronchitis, skin and soft tissue infections, pelvic infections, osteomyelitis, post operative pain.
4.2 Posology and Method of Administration
Dosage depends on the age and renal function of the patient and the severity of the infection.
To minimize potential gastrointestinal intolerance, administer at the start of a meal.
The absorption of Zormox CV 625/1 gm is optimized when taken at the start of a meal.
Tablets to be consumed in whole, not to be broken.
Treatment should not be extended beyond 14 days without review.
Therapy can be started parenterally and continued with an oral preparation.
Zormox CV 625 /1g are not recommended in children of 12 years and under.
Adults and Children over 12 years The usual recommended daily dosage is:
Mild - Moderate infections: One Zormox CV 625 mg tablet every 12 hours
Severe infections: One Zormox CV 1 g tablet every 12 hours OR One Zormox CV 625 mg tablet every 8 hours
Renal Impairment No adjustment in dose is required in patients with creatinine clearance (CrCl) greater than 30 mL/min. The Zormox CV 1g tablet should only be used in patients with a creatinine clearance (CrCl) rate of more than 30 mL/min.
CrCl 10-30 mL/min: One Zormox CV 625 mg tablet every 12 hours
CrCl < 10 mL/min: One Zormox CV 625 mg tablet every 24 hours
Haemodialysis: One Zormox CV 625 mg tablet every 24 hours, plus a further one tablet during dialysis, to be repeated at the end of dialysis (as serum concentrations of both amoxycillin and clavulanic acid are decreased.)
Hepatic Impairment Administer with caution; monitor hepatic function at regular intervals.
4.3 Contraindications
in patients with a history of hypersensitivity to beta-lactams, e.g. penicillins and cephalosporins.
in patients with a previous history of amoxycillin-clavulanate-associated jaundice/hepatic dysfunction.
4.4 Special Warnings and Precautions for use
Before initiating therapy with amoxycillin and clavulanic acid careful enquiry should be made concerning previous hypersensitivity reactions to penicillins, cephalosporins, or other allergens.
Serious and occasionally fatal hypersensitivity reactions (including anaphylactoid and severe cutaneous adverse reactions) have been reported in patients on penicillin therapy. These reactions are more likely to occur in individuals with a history of penicillin hypersensitivity. Hypersensitivity reactions can also progress to Kounis syndrome, a serious allergic reaction that can result in myocardial infarction. Presenting symptoms of such reactions can include chest pain occurring in association with an allergic reaction to amoxycillin and clavulanic acid. Drug-induced enterocolitis syndrome has been reported mainly in children receiving amoxycillin and clavulanic acid. Drug induced enterocolitis syndrome is an allergic reaction with the leading symptom of protracted vomiting (1-4 hours after medicinal product administration) in the absence of allergic skin or respiratory symptoms. Further symptoms could comprise abdominal pain, lethargy, diarrhoea, hypotension or leucocytosis with neutrophilia. In severe cases, drug-induced enterocolitis syndrome can progress to shock. If an allergic reaction occurs, amoxycillin and clavulanic acid therapy must be discontinued and appropriate alternative therapy instituted.
Serious anaphylactic reactions require immediate emergency treatment with adrenaline. Oxygen, intravenous (i.v.) steroids and airway management (including intubation) may also be required.
Haemophagocytic lymphohistiocytosis (HLH)/macrophage activation syndrome (MAS) has been reported in patients receiving amoxycillin-clavulanate. HLH/MAS is a syndrome of pathological immune activation, which can be life threatening. Clinical signs and symptoms of HLH/MAS include fever, rash, neurological symptoms, hepatosplenomegaly, lymphadenopathy, cytopenias, high serum ferritin, hypertriglyceridaemia and abnormalities of liver function and coagulation.
Patients who develop these signs and symptoms should be immediately evaluated and HLH/MAS diagnosis considered. Amoxycillin-clavulanate therapy should be discontinued unless an alternative aetiology for HLH/MAS can be established.
Amoxycillin and clavulanic acid should be avoided if infectious mononucleosis is suspected since the occurrence of a morbilliform rash has been associated with this condition following the use of amoxycillin.
Prolonged use may also occasionally result in overgrowth of non-susceptible organisms. Pseudomembranous colitis has been reported with the use of antibiotics and may range in severity from mild to life-threatening. Therefore, it is important to consider its diagnosis in patients who develop diarrhoea during or after antibiotic use. If prolonged or significant diarrhoea occurs or the patient experiences abdominal cramps, treatment should be discontinued immediately and the patient investigated further.
Abnormal prolongation of prothrombin time [increased International Normalized Ratio (INR)] has been reported rarely in patients receiving amoxycillin and clavulanic acid and oral anticoagulants.
Appropriate monitoring should be undertaken when anticoagulants are prescribed concurrently. Adjustments in the dose of oral anticoagulants may be necessary to maintain the desired level of anticoagulation.
Changes in liver function tests have been observed in some patients receiving amoxycillin and clavulanic acid.
The clinical significance of these changes is uncertain but amoxycillin and clavulanic acid should be used with caution in patients with evidence of hepatic dysfunction.
Cholestatic jaundice, which may be severe, but is usually reversible, has been reported rarely. Signs and symptoms may not become apparent for up to six weeks after treatment has ceased. In patients with renal impairment amoxycillin and clavulanic acid dosage should be adjusted as recommended in 4.2 Posology and Method of Administration.
In patients with reduced urine output, crystalluria has been observed very rarely, predominantly with parenteral therapy. During the administration of high doses of amoxycillin, it is advisable to maintain adequate fluid intake and urinary output in order to reduce the possibility of amoxycillin crystalluria.
4.5 Drug Interactions
Concomitant use of probenecid is not recommended. Probenecid decreases the renal tubular secretion of amoxycillin. Concomitant use with amoxycillin and clavulanic acid may result in increased and prolonged blood levels of amoxycillin but not of clavulanic acid.
Concomitant use of allopurinol during treatment with amoxycillin can increase the likelihood of allergic skin reactions. There are no data on the concomitant use of amoxycillin and clavulanic acid and allopurinol.
In common with other antibiotics, Amoxycillin and clavulanic acid may affect the gut flora, leading to lower oestrogen reabsorption and reduced efficacy of combined oral contraceptives.
In the literature, there are rare cases of increased international normalised ratio in patients maintained on acenocoumarol or warfarin and prescribed a course of amoxycillin. If co administration is necessary, the prothrombin time or international normalised ratio should be carefully monitored with the addition or withdrawal of amoxycillin and clavulanic acid.
In patients receiving mycophenolate mofetil, reduction in pre-dose concentration of the active metabolite mycophenolic acid of approximately 50% has been reported following commencement of oral amoxycillin plus clavulanic acid. The change in pre-dose level may not accurately represent changes in overall MPA exposure.
Penicillins may reduce the excretion of methotrexate causing a potential increase in toxicity.
4.6 Use in Special Population
Pregnancy Reproduction studies in animals (mice and rats at doses up to 10 times the human dose) with orally and parenterally administered amoxycillin and clavulanic acid have shown no teratogenic effects. In a single study in women with preterm, premature rupture of the foetal membrane (pPROM), it was reported that prophylactic treatment with amoxycillin and clavulanic acid may be associated with an increased risk of necrotising enterocolitis in neonates. As with all medicines, use should be avoided in pregnancy, unless considered essential by the physician.
Lactation Amoxycillin and clavulanic acid may be administered during the period of lactation. With the exception of the risk of sensitisation, associated with the excretion of trace quantities in breast milk, there are no known detrimental effects for the breast-fed infant.
4.7 Effects on Ability to Drive and Use Machines
Adverse effects on the ability to drive or operate machinery have not been observed.
4.8 Undesirable Effects
Infections and infestations Common: Mucocutaneous candidiasis
Blood and lymphatic system disorders Rare: Reversible leucopenia (including neutropenia) and thrombocytopenia Very rare: Reversible agranulocytosis and haemolytic anaemia. Prolongation of bleeding time and prothrombin time.
Immune system disorders Very rare: Haemophagocytic lymphohistiocytosis/macrophage activation syndrome, anaphylaxis, angioneurotic oedema, serum sickness-like syndrome, hypersensitivity vasculitis.
Nervous system disorders Uncommon: Dizziness, headache Very rare: Reversible hyperactivity, aseptic meningitis, convulsions. Convulsions may occur in patients with impaired renal function or in those receiving high doses.
Cardiac disorders Very rare: Kounis syndrome
Gastrointestinal disorders Adults: Very common: Diarrhoea; Common: Nausea, vomiting Children: Common: Diarrhoea, nausea, vomiting All populations: Nausea is more often associated with higher oral dosages. If gastrointestinal reactions are evident, they may be reduced by taking Amoxycillin and clavulanic acid at the start of a meal. Uncommon: Indigestion Very rare: Antibiotic-associated colitis (including pseudomembranous colitis and haemorrhagic colitis, drug-induced enterocolitis syndrome, black hairy tongue
Hepatobiliary disorders Uncommon: A moderate rise in AST and/or ALT has been noted in patients treated with beta-lactam class antibiotics, but the significance of these findings is unknown. Very rare: Hepatitis and cholestatic jaundice. These events have been noted with other penicillins and cephalosporins. Hepatic events have been reported predominantly in males and elderly patients and may be associated with prolonged treatment. These events have been very rarely reported in children. Signs and symptoms usually occur during or shortly after treatment but in some cases may not become apparent until several weeks after treatment has ceased. These are usually reversible. Hepatic events may be severe and in extremely rare circumstances, deaths have been reported. These have almost always occurred in patients with serious underlying disease or taking concomitant medications known to have the potential for hepatic effects.
Skin and subcutaneous tissue disorders Uncommon: Skin rash, pruritus, urticaria Rare: Erythema multiforme Very rare: Stevens-Johnson syndrome, toxic epidermal necrolysis, bullous exfoliative dermatitis, acute generalised exanthemous pustulosis (AGEP), drug reaction with eosinophilia and systemic symptoms (DRESS), and symmetrical drug related intertriginous and flexural exanthema (SDRIFE) (baboon syndrome). If any hypersensitivity dermatitis reaction occurs, treatment should be discontinued, linear IgA disease.
Renal and urinary disorders Very rare: Interstitial nephritis, crystalluria
Reporting of Suspected Adverse Reactions Reporting suspected adverse reactions after authorization of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via email to: medico@zorvia.com By reporting side effects, you can help provide more information on the safety of this medicine.
4.9 Overdose
Gastrointestinal symptoms and disturbance of the fluid and electrolyte balances may be evident. Gastrointestinal symptoms may be treated symptomatically with attention to the water electrolyte balance. Amoxycillin crystalluria, in some cases leading to renal failure, has been observed.
Amoxycillin and clavulanic acid can be removed from the circulation by haemodialysis.
5.0 Pharmacological Properties
5.1 Mechanism of Action
Amoxycillin is a semisynthetic antibiotic with a broad spectrum of antibacterial activity against many gram-positive and gram-negative micro-organisms. Amoxycillin is, however, susceptible to degradation by beta-lactamases and therefore the spectrum of activity of amoxycillin alone does not include organisms which produce these enzymes. Clavulanic acid is a beta-lactam, structurally related to the penicillins, which possesses the ability to inactivate a wide range of beta-lactamase enzymes commonly found in micro-organisms resistant to penicillins and cephalosporins. In particular, it has good activity against the clinically important plasmid mediated beta-lactamases frequently responsible for transferred drug resistance. It is generally less effective against chromosomally mediated type 1 beta-lactamases. The presence of clavulanic acid in amoxycillin-clavulanate formulations protects amoxycillin from degradation by beta-lactamase enzymes and effectively extends the antibacterial spectrum of amoxycillin to include many bacteria normally resistant to amoxycillin and other penicillins and cephalosporins. Thus amoxycillin-clavulanate possesses the distinctive properties of a broad-spectrum antibiotic and a beta-lactamase inhibitor.
5.2 Pharmacodynamic Properties
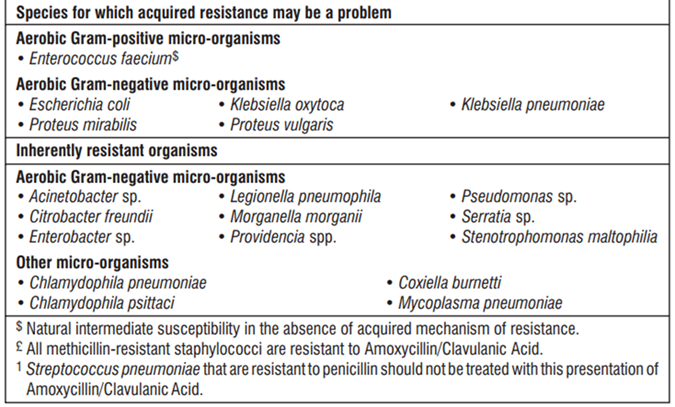
Resistance to many antibiotics is caused by bacterial enzymes which destroy the antibiotic before it can act on the pathogen. The clavulanate in amoxycillin-clavulanate anticipates this defence mechanism by blocking the beta-lactamase enzymes, thus rendering the organism's sensitive to amoxycillin's rapid bactericidal effect at concentrations readily attainable in the body. Clavulanate by itself has little antibacterial activity; however, in association with amoxycillin as amoxycillin-clavulanate it produces an antibiotic agent of broad-spectrum with wide application in hospital and general practice. In the list below, organisms are categorised according to their in vitro susceptibility to amoxycillin-clavulanate.
5.3 Pharmacokinetic Properties
The pharmacokinetics of the two components of amoxycillin-clavulanate are closely matched. Peak serum levels of both occur about 1 hour after oral administration. Absorption of amoxycillin-clavulanate is optimised at the start of a meal.
Doubling the dosage of amoxycillin-clavulanate approximately doubles the serum levels achieved. Both clavulanate and amoxycillin have low levels of serum binding; about 70% remains free in the serum.
6.0 Nonclinical Properties
6.1 Animal Toxicology or Pharmacology
Non-clinical data reveal no special hazard for humans based on studies of safety pharmacology, genotoxicity and toxicity to reproduction
Repeat dose toxicity studies performed in dogs with Amoxycillin/Clavulanic Acid demonstrate gastric irritancy and vomiting, and discoloured tongue.
Carcinogenicity studies have not been conducted with Amoxycillin/Clavulanic Acid.
7.0 Description
Zormox CV 625/1 gm (beta-lactam antibacterial penicillin coformulated with a beta-lactamase inhibitor) is an antibiotic agent with a notably broad spectrum of activity against the commonly occurring bacterial pathogens in general practice and hospital. The beta-lactamase inhibitory action of clavulanate extends the spectrum of amoxycillin to embrace a wider range of organisms, including many resistant to other beta-lactam antibiotics.
8. Pharmaceutical particulars
8.1 Incompatibilities
Not applicable
8.2 Shelf-Life
Refer on pack
8.3 Packaging Information
Refer on pack
8.4 Storage and Handling Instructions
Store protected from moisture, at a temperature not exceeding 25°C. Keep all medicines out of reach of children
9.0 Patient Counselling Information
Patients should be informed that Zormox CV 625/1 gm may be taken every 8 hours or every 12 hours, depending on the dose prescribed. Each dose should be taken with a meal or snack to reduce the possibility of gastrointestinal upset.
Patients should be counseled that antibacterial drugs, including Zormox CV 625/1 gm, should only be used to treat bacterial infections. They do not treat viral infections (e.g., the common cold).
When Zormox CV 625/1 gm is prescribed to treat a bacterial infection, patients should be told that although it is common to feel better early in the course of therapy, the medication should be taken exactly as directed. Skipping doses or not completing the full course of therapy may : (1) decrease the effectiveness of the immediate treatment, and (2) increase the likelihood that bacteria will develop resistance and will not be treatable by Zormox CV 625/1 gm or other antibacterial drugs in the future.
Counsel patients that diarrhea is a common problem caused by antibacterials, and it usually ends when the antibacterial is discontinued. Sometimes after starting treatment with antibacterials, patients can develop watery and bloody stools (with or without stomach cramps and fever) even as late as 2 or more months after having taken their last dose of the antibacterial. If diarrhea is severe or lasts more than 2 or 3 days, patients should contact their physician.
Patients should be aware that Zormox CV 625/1 gm contains a penicillin class drug product that can cause allergic reactions in some individuals.