To be sold on retail on prescription of a Registered Medical Practitioner only.
Prescribing Information
1.0 Generic Name
Levodropropizine syrup
2.0 Qualitative and Quantitative Composition
Each 5 ml contains: Levodropropizine IP……………………………….30 mg
3.0 Dosage Form and Strength
Syrup 30 mg/5 ml
4.0 Clinical Particulars
4.1 Therapeutic Indications
Symptomatic treatment of non-productive cough.
4.2 Posology and Method of Administration
Adults and children from 12 years and older Maximum 60 mg levodropropizine (10 ml syrup), three times daily. The time between administrations should be at least 6 hours.
Children over 2 years 1 mg/kg bodyweight given three times daily for a total daily doses of 3mg/kg body weight at intervals of at least 6 hours. Levodropropizine syrup contraindicated in children below 2 years.
Elderly In elderly patients, levodropropizine is used with caution; a risk of changed pharmacokinetics linked to age can be present.
Renal and Hepatic Impairment In case of severe renal (creatin clearance below 35ml/min) or in case of severe hepatic failure, the benefit-risk ratio should be taken into consideration.
Method of administration: Preferably, the syrup will be taken away from meals with an interval of at least 6 hours between administrations. The period of treatment should remain brief; treatment should be discontinued as soon as the symptoms have disappeared.
4.3 Contraindications
Known hypersensitivity to the active substance or to any of the excipients listed in the formulation.
Bronchorrhoea or disturbed muco-ciliary function (Kartagener syndrome, bronchial dyskinesia).
Pregnancy and lactation.
Children below 2 years.
4.4 Special Warnings and Precautions for use
Before starting treatment with a cough syrup, cough-underlying causes requiring a specific treatment should be investigated. It is not coherent to administer a cough preparation combined with mucolytics or expectorants.
In elderly patients, levodropropizine is used with caution; a risk of changed pharmacokinetics linked to age can be present.
In case of severe renal (creatin clearance below 35ml/min) or in case of severe hepatic failure, the benefit-risk ratio should be taken into consideration.
In the absence of studies to determine the influence of food on the absorption of levodropropizine, advice is given to take the syrup away from meals.
4.5 Drug Interactions
Clinical studies have not revealed interactions following simultaneous administration of medicines used to treat bronchopulmonary diseases.
Patients sensitive to sedative medication should be careful when using these medicines combined with levodropropizine.
4.6 Use in special populations
Pregnancy There are not enough clinical data studying the use of levodropropizine during pregnancy to evaluate the potential toxicity. Tusvia syrup is contraindicated during pregnancy.
Lactation In animal studies it was demonstrated that levodropropizine is excreted in maternal milk. Therefore, Tusvia syrup is contra-indicated during breast feeding.
Fertility There are no data available.
4.7 Effects on Ability to Drive and Use Machines
In exceptional cases, somnolence and vertigo have been reported. Caution is advised when driving or operating a machine.
Reporting of Suspected Adverse Reactions Reporting suspected adverse reactions after authorization of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via email to: medico@zorvia.com By reporting side effects, you can help provide more information on the safety of this medicine.
4.9 Overdose
Significant undesirable effects have not been observed following ingestion of a single dose up to 240 mg or following ingestion of multiple 120 mg doses, 3 times daily for 8 consecutive days. In case of an overdose, a temporary transitional tachycardia can be expected. General measures for treating a drug overdose apply (gastric lavage, activated charcoal, giving parenteral fluid).
5.0 Pharmacological Properties
5.1 Mechanism of action
Levodropropizine inhibit the cough reflex by acting on the peripheral receptors and their afferent conductors. Levodropropizine inhibits the C-fibers of the vagus nerves and modulate the sensory neuropeptides production in the respiratory tract, involved in the cough reflex. Levodropropizine has a dose-dependent and short-term local anaesthetic activity. It also has a mild analgesic and an antihistaminic action.
5.2 Pharmacodynamic properties
Levodropropizine is a peripherally acting antitussive working at tracheobronchial level. The peripheral action has been demonstrated in animal studies. Its mechanism provides this drug antitussive properties against cough associated to different lung pathologies, but without relevant central side effects. Levodropropizine inhibits bronchospasms induced by histamine, serotonin and bradykinin. Levodropropizine exerts its antitussive effect through an inhibitory action at the level of the airway sensory nerves involving modulation of sensitive C-fibers and release of neuropeptides.
5.3 Pharmacokinetic properties
Absorption Bioavailability of levodropropizine was found to be greater than 75% after oral administration. Plasma protein binding rate was lower (11-14%).
Distribution In human, oral levodropropizine was rapidly absorbed and distributed throughout the body.
Biotransformation There is no data about the specific site of metabolism of levodropropizine either in the liver or in other sites.
Elimination Plasma elimination half-life of levodropropizine is approximately 1-2 hours. Its excretion is mainly in the urine. Elimination of the active substance is either in the form of both unchanged and conjugated or free levodropropizine or in conjugated p-hydroxy-levodropropizine metabolites. Elimination of the active substance and its metabolites in 48 hours approximates to 35% of the administered dose. Results of the repeat dose studies have demonstrated that 8 days of treatment (3 times a day) did not alter the elimination characteristics of the drug and therefore accumulation or metabolic auto-induction were unlikely.
6.0 Nonclinical Properties
6.1 Animal Toxicology or Pharmacology
Acute oral toxicity is 886.5 mg/kg, 1287mg/kg and 2492 mg/kg, respectively in rats, mice and guinea pigs. In guinea pigs, the therapeutic index calculated as the ratio of LD50/ED50after oral administration was 16 to 53, depending on the cough induction model. Toxicity tests for repeated oral administrations have shown that the daily dose without toxic effect corresponds to 24 mg/kg.
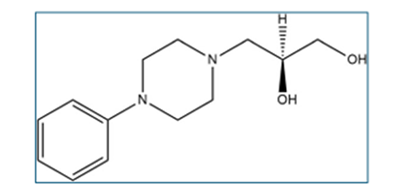
7.0 Description
Levodropropizine belongs to class of medicines called antitussives. Its chemical name is (2S)-3-(4-Phenylpiperazin-1-yl)propane-1,2-diol. Molecular formula: C13H20N2O2 Molecular weight: 236.315 g/mol
8.0 Pharmaceutical Particulars
8.1 Incompatibilities
Not applicable
8.2 Shelf-Life
Refer on pack
8.3 Packaging Information
100 ml Bottle
8.4 Storage and Handling Instructions
Store at a temperature not exceeding 30°C. Protect from light.
9.0 Patient Counselling Information
Take this medicine exactly as prescribed by your doctor. Do not exceed the recommended dose or duration.
This syrup is used for dry (non-productive) cough. Do not use it along with expectorants or mucolytics unless advised by a doctor.
Maintain a minimum interval of 6 hours between doses and preferably take it away from meals.
Do not use in children below 2 years and use with caution in elderly patients.
Inform your doctor if you have kidney or liver problems before taking this medicine.
Do not use during pregnancy or breastfeeding. Consult your doctor if you are pregnant or planning pregnancy.
This medicine may cause drowsiness or dizziness in some patients. Avoid driving or operating machinery if affected.
Stop the medicine and consult your doctor if you experience allergic reactions, breathing difficulty, or unusual symptoms.
Treatment should be short-term and discontinued once symptoms improve. If cough persists, seek medical advice.