To be sold on retail on prescription of a Registered Medical Practitioner only.
Prescribing Information
Oseltamivir Capsules IP 75 mg
1.0 Generic Name
Oseltamivir Capsules IP
2.0 Qualitative and Quantitative Composition
Each hard gelatin capsule contains: Oseltamivir Phosphate IP eq. to Oseltamivir…75mg Excipients…………………………………………………. q.s. Approved colours used in empty hard gelatin capsule shells
3.0 Dosage Form and Strength
Hard gelatin capsule, 75mg
4.0 Clinical Particulars
4.1 Therapeutic Indications
For influenzae
4.2 Posology and Method of Administration
Adults, and adolescents 13 years and over
Treatment of Influenza The recommended oral dose is 75 mg oseltamivir twice daily for 5 days for adolescents (13 to 17 years of age) and adults.
Body Weight
Recommended dose for 5 days
Recommended dose for 10 days Immunocompromised Patients
> 40 kg
75 mg twice daily
75 mg twice daily
Treatment should be initiated as soon as possible within the first two days of onset of symptoms of influenza.
Post-exposure prevention The recommended dose for prevention of influenza following close contact with an infected individual is 75 mg oseltamivir once daily for 10 days for adolescents (13 to 17 years of age) and adults.
Body Weight
Recommended dose for 10 days
Recommended dose for 10 days Immunocompromised Patients
> 40 kg
75 mg once daily
75 mg once daily
Prevention during an influenza epidemic in the community The recommended dose for prevention of influenza during a community outbreak is 75 mg oseltamivir once daily for up to 6 weeks (or up to 12 weeks in immuno-compromised patients).
Paediatric population Children 1 to 12 years of age
Treatment of Influenza The following weight-adjusted dosing regimens are recommended for treatment of infants and children 1year of age or older:
Body Weight
Recommended dose for 5 days
Recommended dose for 10 days Immunocompromised Patients
> 40 kg
75 mg twice daily
75 mg twice daily
Treatment should be initiated as soon as possible within the first two days of onset of symptoms of influenza.
Post-exposure prevention The recommended post-exposure prevention dose of Oseltamivir is:
Body Weight
Recommended dose for 10 days
Recommended dose for 10 days For Immunocompromised Patients
> 40 kg
75 mg once daily
75 mg once daily
Prevention during an influenza epidemic in the community Prevention during an influenza epidemic has not been studied in children below 12 years of age.
Special populations Hepatic impairment: No dose adjustment is required either for treatment or for prevention in patients with hepatic dysfunction. No studies have been carried out in paediatric patients with hepatic disorder.
Renal impairment Treatment of influenza: Dose adjustment is recommended for adults and adolescents (13 to 17 years of age) with moderate or severe renal impairment. Recommended doses are detailed in the table below:
Creatinine clearance
Recommended dose for treatment
> 60 (ml/min)
75 mg twice daily
> 30 to 60 (ml/min)
30 mg twice daily
> 10 to 30 (ml/min)
30 mg once daily
≤ 10 (ml/min)
Not recommended (no data available)
Haemodialysis patients
30 mg after each haemodialysis session
Peritoneal dialysis patients
30 mg single dose
Prevention of influenza: Dose adjustment is recommended for adults and adolescents (13 to 17 years of age) with moderate or severe renal impairment as detailed in the table below:
Creatinine clearance
Recommended dose for prevention
> 60 (ml/min)
75 mg once daily
> 30 to 60 (ml/min)
30 mg once daily
> 10 to 30 (ml/min)
30 mg every second day
≤ 10 (ml/min)
Not recommended (no data available)
Haemodialysis patients
30 mg after every second haemodialysis session
Peritoneal dialysis patients
30 mg once weekly
There is insufficient clinical data available in infants and children (12 years of age and younger) with renal impairment to be able to make any dosing recommendation.
Elderly No dose adjustment is required, unless there is evidence of moderate or severe renal impairment.
Immunocompromised patients Treatment: For treatment of influenza, the recommended duration for immunocompromised patients is 10 days. No dose adjustment is necessary. Treatment should be initiated as soon as possible within the first two days of onset of symptoms of influenza. Seasonal prophylaxis: Longer duration of seasonal prophylaxis up to 12 weeks has been evaluated in immuno-compromised patients.
4.3 Contraindications
Hypersensitivity to the active substance or to any of the excipients present in formulation
4.4 Special Warnings and Precautions for use
Oseltamivir is effective only against illness caused by influenza viruses. There is no evidence for efficacy of oseltamivir in any illness caused by agents other than influenza viruses.
Oseltamivir is not a substitute for influenza vaccination. Use of Oseltamivir must not affect the evaluation of individuals for annual influenza vaccination. The protection against influenza lasts only as long as Oseltamivir is administered. Oseltamivir should be used for the treatment and prevention of influenza only when reliable epidemiological data indicate that influenza virus is circulating in the community.
Susceptibility of circulating influenza virus strains to oseltamivir has been shown to be highly variable. Therefore, prescribers should take into account the most recent information available on oseltamivir susceptibility patterns of the currently circulating viruses when deciding whether to use Oseltamivir.
Severe concomitant condition No information is available regarding the safety and efficacy of oseltamivir in patients with any medical condition sufficiently severe or unstable to be considered at imminent risk of requiring hospitalisation.
Immunocompromised patients The efficacy of oseltamivir in either treatment or prophylaxis of influenza in immunocompromised patients has not been firmly established.
Cardiac / respiratory disease Efficacy of oseltamivir in the treatment of subjects with chronic cardiac disease and/or respiratory disease has not been established. No difference in the incidence of complications was observed between the treatment and placebo groups in this population.
Paediatric population No data allowing a dose recommendation for premature children (<36 weeks post-conceptual age) are currently available.
Severe renal impairment Dose adjustment is recommended for both treatment and prevention in adolescents (13 to 17 years of age) and adults with severe renal impairment. There is insufficient clinical data available in infants and children (1 year of age or older) with renal impairment to be able to make any dosing recommendation.
Neuropsychiatric events Neuropsychiatric events have been reported during administration of Oseltamivir in patients with influenza, especially in children and adolescents. These events are also experienced by patients with influenza without oseltamivir administration. Patients should be closely monitored for behavioural changes, and the benefits and risks of continuing treatment should be carefully evaluated for each patient.
4.5 Drug Interactions
Pharmacokinetic properties of oseltamivir, such as low protein binding and metabolism independent of the CYP450 and glucuronidase systems, suggest that clinically significant drug interactions via these mechanisms are unlikely.
Probenecid No dose adjustment is required when co-administering with probenecid in patients with normal renal function. Co-administration of probenecid, a potent inhibitor of the anionic pathway of renal tubular secretion, results in an approximate 2-fold increase in exposure to the active metabolite of oseltamivir.
Amoxicillin Oseltamivir has no kinetic interaction with amoxicillin, which is eliminated via the same pathway, suggesting that oseltamivir interaction with this pathway is weak.
Renal elimination Clinically important drug interactions involving competition for renal tubular secretion are unlikely, due to the known safety margin for most of these substances, the elimination characteristics of the active metabolite (glomerular filtration and anionic tubular secretion) and the excretion capacity of these pathways. However, care should be taken when prescribing oseltamivir in subjects when taking co-excreted agents with a narrow therapeutic margin (e.g. chlorpropamide, methotrexate, phenylbutazone).
Additional information No pharmacokinetic interactions between oseltamivir or its major metabolite have been observed when co-administering oseltamivir with paracetamol, acetylsalicylic acid, cimetidine, antacids (magnesium and aluminium hydroxides and calcium carbonates), rimantadine or warfarin (in subjects stable on warfarin and without influenza).
4.6 Use in Special Population
Pregnancy Influenza is associated with adverse pregnancy and fetal outcomes, with a risk of major congenital malformations, including congenital heart defects. A large amount of data on oseltamivir exposure of pregnant women from post- marketing reports and observational studies (more than 1000 exposed outcomes during the first trimester) indicate no malformative nor feto/neonatal toxicity by oseltamivir. However, in one observational study, while the overall malformation risk was not increased, the results for major congenital heart defects diagnosed within 12 months of birth were not conclusive. In this study, the rate of major congenital heart defects following oseltamivir exposure during the first trimester was 1.76% (7 infants out of 397pregnancies) compared to 1.01% in unexposed pregnancies from the general population (Odds Ratio 1.75, 95%Confidence Interval 0.51 to 5.98). The clinical significance of this finding is not clear, as the study had limited power. Additionally, this study was too small to reliably assess individual types of major malformations; moreover, women exposed to oseltamivir and women unexposed could not be made fully comparable, in particular whether or not they had influenza. Animal studies do not indicate reproductive toxicity. The use of Oseltamivir may be considered during pregnancy if necessary and after considering the available safety and benefit information, and the pathogenicity of the circulating influenza virus strain.
Breastfeeding In lactating rats, oseltamivir and the active metabolite are excreted in milk. Very limited information is available on children breast-fed by mothers taking oseltamivir and on excretion of oseltamivir in breast milk. Limited data demonstrated that oseltamivir and the active metabolite were detected in breast milk, however the levels were low, which would result in a subtherapeutic dose to the infant. Considering this information, the pathogenicity of the circulating influenza virus strain and the underlying condition of the breastfeeding woman, administration of oseltamivir may be considered, where there are clear potential benefits to breastfeeding mothers.
Fertility There is no evidence that Oseltamivir has an effect on male or female fertility.
4.7 Effects on Ability to Drive and Use Machines
Oseltamivir has no influence on the ability to drive and use machines
General disorders and administration site conditions
Pain, Dizziness (incl. vertigo), Fatigue, Pyrexia, Pain in limb
Reporting of Suspected Adverse Reactions Reporting suspected adverse reactions after authorization of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via email to: medico@zorvia.com By reporting side effects, you can help provide more information on the safety of this medicine.
4.9 Overdose
Reports of overdoses with Oseltamivir have been reported from clinical trials and during postmarketing experience. In the majority of cases reporting overdose, no adverse reactions were reported. Adverse reactions reported following overdose were similar in nature to those observed with therapeutic doses of Oseltamivir.
5.0 Pharmacological Properties
5.1 Mechanism of Action
Oseltamivir is an antiviral drug with activity against influenza virus.
5.2 Pharmacodynamic Properties
Oseltamivir phosphate is a pro-drug of the active metabolite (oseltamivir carboxylate). The active metabolite is a selective inhibitor of influenza virus neuraminidase enzymes, which are glycoproteins found on the virion surface. Viral neuraminidase enzyme activity is important both for viral entry into uninfected cells and for the release of recently formed virus particles from infected cells, and for the further spread of infectious virus in the body.
Oseltamivir carboxylate inhibits influenza A and B neuraminidases in vitro. Oseltamivir phosphate inhibits influenza virus infection and replication in vitro. Oseltamivir given orally inhibits influenza A and B virus replication and pathogenicity invivo in animal models of influenza infection at antiviral exposures similar to that achieved in man with 75 mg twice daily.
Antiviral activity of oseltamivir was supported for influenza A and B by experimental challenge studies in healthy volunteers.
Neuraminidase enzyme IC50 values for oseltamivir for clinically isolated influenza A ranged from 0.1 nM to 1.3 nM, andfor influenza B was 2.6 nM. Higher IC50 values for influenza B, up to a median of 8.5 nM, have been observed in studies.
5.3 Pharmacokinetic Properties
Absorption Oseltamivir is readily absorbed from the gastrointestinal tract after oral administration of oseltamivir phosphate (pro-drug) and is extensively converted by predominantly hepatic esterases to the active metabolite (oseltamivir carboxylate). At least 75 % of an oral dose reaches the systemic circulation as the active metabolite. Exposure to the pro-drug is less than 5 % relative to the active metabolite. Plasma concentrations of both pro-drug and active metabolite are proportional to dose and are unaffected by co-administration with food.
Distribution The mean volume of distribution at steady state of the oseltamivir carboxylate is approximately 23 litres in humans, a volume equivalent to extracellular body fluid. Since neuraminidase activity is extracellular, oseltamivir carboxylate distributes to all sites of influenza virus spread. The binding of the oseltamivir carboxylate to human plasma protein is negligible (approximately 3 %).
Biotransformation Oseltamivir is extensively converted to oseltamivir carboxylate by esterases located predominantly in the liver. In vitro studies demonstrated that neither oseltamivir nor the active metabolite is a substrate for, or an inhibitor of, the major cytochrome P450 isoforms. No phase 2 conjugates of either compound have been identified in vivo.
Elimination Absorbed oseltamivir is primarily (> 90 %) eliminated by conversion to oseltamivir carboxylate. It is not further metabolised and is eliminated in the urine. Peak plasma concentrations of oseltamivir carboxylate decline with a half-life of 6 to 10 hours in most subjects. The active metabolite is eliminated entirely by renal excretion. Renal clearance (18.8l/h) exceeds glomerular filtration rate (7.5 l/h) indicating that tubular secretion occurs in addition to glomerular filtration. Less than 20 % of an oral radiolabelled dose is eliminated in faeces.
6.0 Nonclinical Properties
6.1 Animal Toxicology or Pharmacology
Preclinical data reveal no special hazard for humans based on conventional studies of safety pharmacology, repeated-dose toxicity and genotoxicity. Results of the conventional rodent carcinogenicity studies showed a trend towards a dose-dependent increase in the incidence of some tumours that are typical for the rodent strains used. Considering the margins of exposure in relation to the expected exposure in the human use, these findings do not change the benefit-risk of oseltamivir in its adopted therapeutic indications.
Teratology studies have been conducted in rats and rabbits at doses of up to 1,500 mg/kg/day and 500 mg/kg/day, respectively. No effects on foetal development were observed. A rat fertility study up to a dose of 1,500 mg/kg/day demonstrated no adverse reactions on either sex. In pre- and post-natal rat studies, prolonged parturition was noted at 1,500 mg/kg/day: the safety margin between human exposure and the highest no-effect dose (500 mg/kg/day) in rats is480-fold for oseltamivir and 44-fold for the active metabolite, respectively. Foetal exposure in the rats and rabbits was approximately 15 to 20 % of that of the mother.
In lactating rats, oseltamivir and the active metabolite are excreted in the milk. Limited data indicate that oseltamivir and the active metabolite are excreted in human milk. Extrapolation of the animal data provides estimates of 0.01 mg/day and 0.3 mg/day for the respective compounds.
A potential for skin sensitisation to oseltamivir was observed in a "maximisation" test in guinea pigs. Approximately 50 % of the animals treated with the unformulated active substance showed erythema after challenging the induced animals. Reversible irritancy of rabbits' eyes was detected.
Whereas very high oral single doses of oseltamivir phosphate salt, up to the highest dose tested (1,310 mg/kg), had no adverse reactions in adult rats, such doses resulted in toxicity in juvenile 7-day-old rat pups, including death. These reactions were seen at doses of 657 mg/kg and higher. At 500 mg/kg, no adverse reactions were seen, including upon chronic treatment (500 mg/kg/day administered from 7 to 21 days post-partum).
7.0 Description
TamibidTM-75 (oseltamivir phosphate) is an influenza neuraminidase inhibitor (NAI), which is available as Capsules containing 75 mg of oseltamivir for oral use, in the form of oseltamivir phosphate.
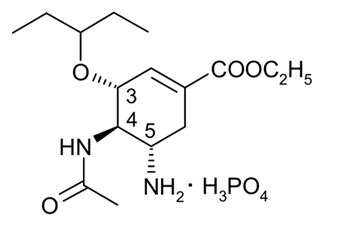
Chemical name: (3R,4R,5S) ‐4‐acetylamino‐5‐amino‐3(1 ethylpropoxy) ‐1‐cyclohexene‐1‐carboxylic acid, ethyl ester, phosphate (1:1). Molecular formula: C16H28N2O4 (free base). Molecular weight: 312.4 for oseltamivir free base and 410.4 for oseltamivir phosphate salt
8. Pharmaceutical particulars
8.1 Incompatibilities
None.
8.2 Shelf-Life
Refer on pack.
8.3 Packaging Information
As per carton.
8.4 Storage and Handling Instructions
Store below 25°C, protect from light & moisture. Keep out of reach of children
9.0 Patient Counselling Information
Serious Skin/Hypersensitivity Reactions: Advise patients and/or caregivers of the risk of severe allergic reactions (including anaphylaxis) or serious skin reactions. Instruct patients and/or caregiver to stop TamibidTM-75 and seek immediate medical attention if an allergic‐like reaction occurs or is suspected.
Neuropsychiatric Events: Advise patients and/or caregivers of the risk of neuropsychiatric events in TamibidTM-75 treated patients with influenza and instruct patients to contact their physician if they experience signs of abnormal behaviour while receiving TamibidTM-75.
Important Dosing Information: Instruct patients to begin treatment with Oseltamivir as soon as possible from the first appearance of flu symptoms, within 48 hours of onset of symptoms. Similarly, instruct patients to start taking TamibidTM-75 for prevention as soon as possible after exposure. Instruct patients to take any missed doses as soon as they remember, except if it is near the next scheduled dose (within 2 hours) and then continue to take Oseltamivir at the usual times.
Influenza Vaccines: Instruct patients that TamibidTM-75 is not a substitute for receiving an annual flu vaccination. Patients should continue receiving an annual flu vaccination according to guidelines on immunization practices. Because of the potential for TamibidTM-75 to inhibit replication of live attenuated influenza vaccine (LAIV) and possibly reduce efficacy of LAIV, avoid administration of LAIV within 2 weeks or 48 hours after TamibidTM-75 administration, unless medically necessary.